

#NephJC chat Tuesday Feb 9th 9 pm Eastern
Wednesday Feb 10th 8 pm GMT, 12 noon Pacific
Nephrol Dial Transplant. 2015 Dec 24. pii: gfv407. [Epub ahead of print]
Prevalence and distribution of (micro)albuminuria in toddlers.
Gracchi V, van den Belt SM, Küpers LK, Corpeleijn E, de Zeeuw D, Heerspink HJ.
Thanks to the folks at NDT for making this article free for #NephJC, available at this link
Summary by Pascale Lane, cross-posted from Whizbang
So-called microalbuminuria first gained attention as a predictor or marker of diabetic kidney disease. We now know that it is not as good as we thought for that condition, but it is associated with renal and cardiovascular disease risk in adults. Is shedding extra albumin in the urine a risk marker or, perhaps, does it contribute to the development of these conditions? After all, these are major causes of morbidity and mortality.
Could it be that microalbuminuria precedes any of the other stuff? Are we born this way?
The first question to answer is the prevalence of microalbuminuria in children. A group in The Netherlands organized a cohort study over the first two years of life in its general population, the Groningen Expert Center for Kids with Obesity (GECKO). All children born in Drenthe, a northern Dutch province, were eligible for enrollment From April 2006 through April 2007. The primary goal of this study was to identify factors associated with overweight. Data included pregnancy complications, birth weight, placenta weight, and longitudinal anthropomorphic measurements through 5 years of age. Lifestyle and environment factors were assessed by questionnaires beginning in the last trimester of pregnancy. Over the 2-year enrollment period 4778 eligible births were recorded. For this study, a urinary albumin measurement had to be performed; 1352 children did this and were included in their analysis. Children with urine studies did not differ from the overall population for any variable studied.
Their method of urine collection sparks some controversy. Two-year-olds usually do not pee in a cup on command. Sticking a plastic baggy on the perineum requires some skill so that it hangs on long enough for the collection but does not get contaminated by stool. The investigators gave the parents a cotton wool pad to place in the diaper and mail back into the center within 24 hrs. They compared this method to voided urines and found acceptable performance for their method with bias -14 mg/dL albumin, precision 31.3 mg/L, and accuracy 48.1%. Contact with cotton is known to decrease albumin levels within 15 minutes by an average of 40% with high variability. A nice review of issues with pediatric urine collection can be found at another link.
The standard clinical measurement of microalbuminuria is the albumin:creatinine ratio to correct for the amount of hydration. The median ratio in this study was 14.0 mg/g creatinine. The 75th percentile was 25.6 and the 95th percentile 89.3 mg/g, respectively. Based on the current criteria for microalbuminuria (ratio > 30 mg/g), 23.4% of their kids had microalbuminuria. However, this normal range comes from adult data. Toddlers often have lower creatinine levels because of their lower muscle mass. More study will be needed to determine a level of risk in this population.
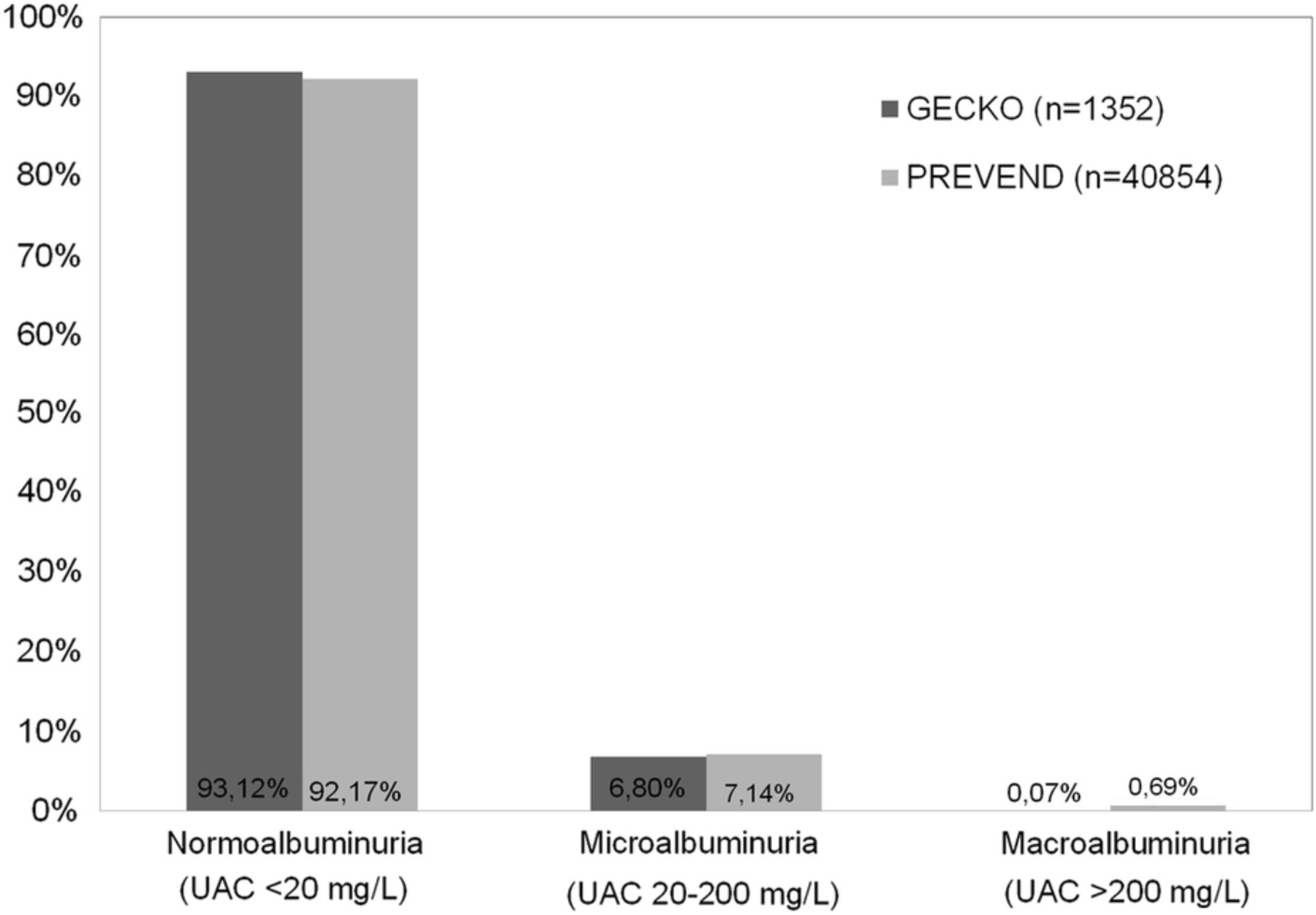
Figure 3 from Gracchi et al: Prevalence of different levels of urinary albumin concentration (UAC) in the general toddler population (GECKO) when compared with the general adult population (PREVEND) in the northern Dutch provinces.
The authors had data from another regional adult study (PREVEND) for comparisons, although it used concentration of albumin rather than the ratio. Using albumin concentrations, 6.9% of toddlers met criteria for microalbuminuria, similar to levels seen in healthy adults overall (Fig 3, right). This is especially true for young adults (Fig 4, below).

FIGURE 4 from Gracchi et al:
Prevalence of increased albuminuria (UAC ≥ 20 mg/L) in different age ranges in the general population of the Dutch northern provinces (data from the GECKO and PREVEND cohorts).
Effects of prenatal and early life factors to promote disease later in life have been proposed for years, most famously by Barker in the relationship between low birth weight and later cardiovascular risk. No association could be demonstrated with birthweight, gestation age, impaired placental growth, gestational hypertension, or smoking during pregnancy, providing no support for the Barker hypothesis.
Other issues include the use of a single specimen for determination of albuminuria. A variety of factors can cause transient urinary abnormalities. Repeated elevations over weeks to months are required for clinical use at this time.
While not definitive, this study provides valuable information on microalbuminuria in toddlers. Might we be born with differences in endothelial function, or in other kidney structures, that make our kidneys leaky and predispose us to later cardiovascular disease? Only time, and further study, will tell.
#NephJC chat Tuesday Feb 9th 9 pm Eastern
Wednesday Feb 10th 8 pm GMT, 12 noon Pacific