
#NephJC Chat
Tuesday Sept 25, 9 pm Eastern
Wednesday Sept 26, 8 pm BST, 12 noon Pacific
J Am Soc Nephrol. 2018 Aug;29(8):2200-2212. doi: 10.1681/ASN.2018020151. Epub 2018 Jun 15.
Decline in Kidney Function among Apparently Healthy Young Adults at Risk of Mesoamerican Nephropathy.
Gonzalez-Quiroz M, Smpokou ET, Silverwood RJ, Camacho A, Faber D, Garcia BR, Oomatia A, Hill M, Glaser J, Le Blond J, Wesseling C, Aragon A, Smeeth L, Pearce N, Nitsch D, Caplin B.
PMID: 29907699 Full Text at JASN (free for 2 weeks)


Introduction
In the western lowlands of Nicaragua, in a region of vast sugarcane fields, sits the tiny community of La Isla.
Kidney disease has killed so many men here that locals now call their community not simply La Isla, "The Island", but La Isla de las Viudas "The Island of the Widows.
The story of this land, narrated by Kate Sheehy, paints the morbid picture which scientific numbers fail to achieve.
Mesoamerican nephropathy (MeN), also called chronic kidney disease of unknown cause (CKDu), refers to CKD that presents in young, agricultural workers primarily in Central America, India, Sri Lanka, and other tropical countries. The disease has been reported in epidemic proportions and is associated with substantial morbidity and early mortality in young and middle-aged individuals.
Characteristics of CKDu
Traditional risk factors such as diabetes and hypertension are absent.
Predominantly affects men
Victims work in hot, tropical agricultural communities (but is seen in other occupations too)
Largely asymptomatic
Elevated creatinine without (significant) proteinuria
The disease entity was first described in a paper from El Salvador, where a large proportion of patients initiated on dialysis had no obvious cause of CKD. Since then, CKDu has been reported from Sri Lanka, several Central American countries, the state of Andhra Pradesh in India, and the El-Minia Governorate in Egypt. In Sri Lanka it was described as chronic interstitial nephritis in agricultural communities (CINAC).
Varying rates of prevalence and incidence of CKDu have been reported in the literature. This is likely to be influenced by local biopsy practices as well as environmental, socioeconomic, and genetic factors.
Central America:
El Salvador – Several surveys epidemiological studies have been performed with reported prevalence ranging from 18% to 30% in coastal areas. Similar numbers have been reported from Nicaragua.
South Asia
Sri Lanka: The age-standardised prevalence of CKDu was 12.9% in men and 16.9% in women. Severe stages of CKDu were more frequent in men.
India: Data from the CKD registry (52,273 adult patients) showed that CKD of undetermined etiology (16%) was a common cause of CKD, second only to Diabetic Nephropathy (31%)
Africa:
Egypt: In a study of 800 patients, CKDu was found to be the commonest cause of CKD (27%.)
The information about CKDu in the affected areas is limited and it is not clear that the etiology of the kidney disease is the same in all locations. Different risk factors have been described -
Heat stress with repeated dehydration and rehydration (Read this previous Nephjc coverage)
Agricultural and physically demanding work in a hot climate
Consumption of sugar-containing rehydration drinks
Hyperuricemia
Infectious agents
Leptospirosis
UTI / Pyelonephritis
Toxins (none have been proven)
Exposure to pesticides
Quality of water
Excessive use of nonsteroidal anti-inflammatory agents
Male sex
Low body mass
Lower socioeconomic class or poverty

Altitude and occupational risks factors have received more attention in Central America whereas extensive chemical monitoring was recently reported in Sri Lanka.
CKDu is a serious public health problem. It disproportionately affects poor, rural, male farmers living in hot climates. The disease is not well understood despite more than 20 years of study. CKDu is a terminal diagnosis in regions where dialysis and kidney transplant are not widely available.

The Study
Aim
The current study investigated the natural history of disease, specifically early loss of kidney function, along with risk factors associated with decline in eGFR.
Methods
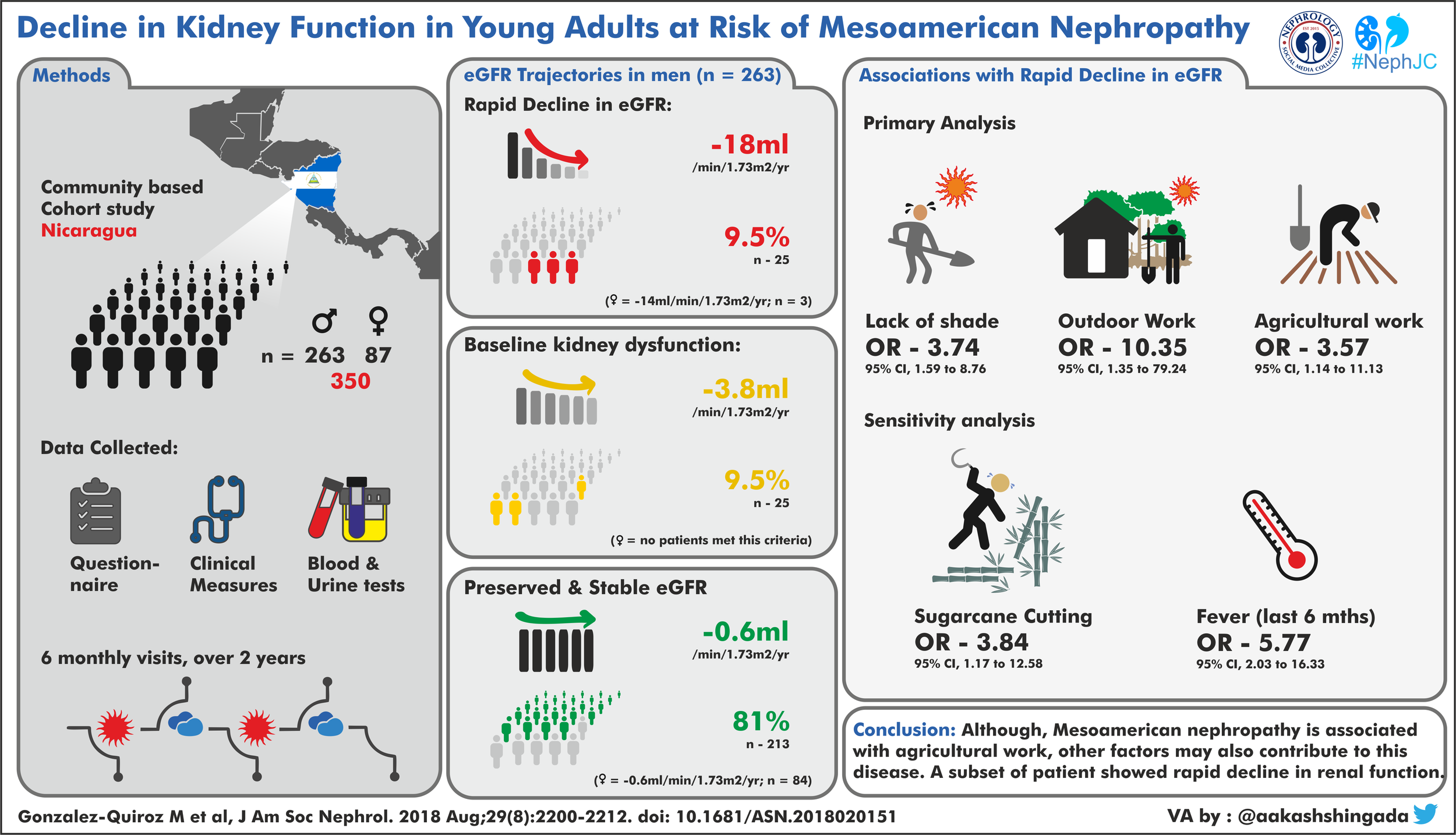
A 2-year longitudinal, community-based study of an initially healthy, young, rural population, in northwest Nicaragua (Leon and Chinandega regions).
Inclusion:
Age 18–30 years
All men (Men have been reported to suffer more CKDu).
Women: selected at random (leading to a male-to-female ratio of 3:1)
Exclusion:
All potential participants with a self-reported diagnosis of CKD, diabetes, or hypertension were excluded.
Study Period:
2 years, beginning in Nov 2014
Methodology:
6 monthly visits for a total of 4 visits were made. (See Figure 3)
The investigators collected Questionnaire data, clinical measurements, and biosamples at baseline and then every 6 months until November 2016. Biosamples included: serum creatinine and cystatin C. Urine albumin, creatinine, urinalysis.
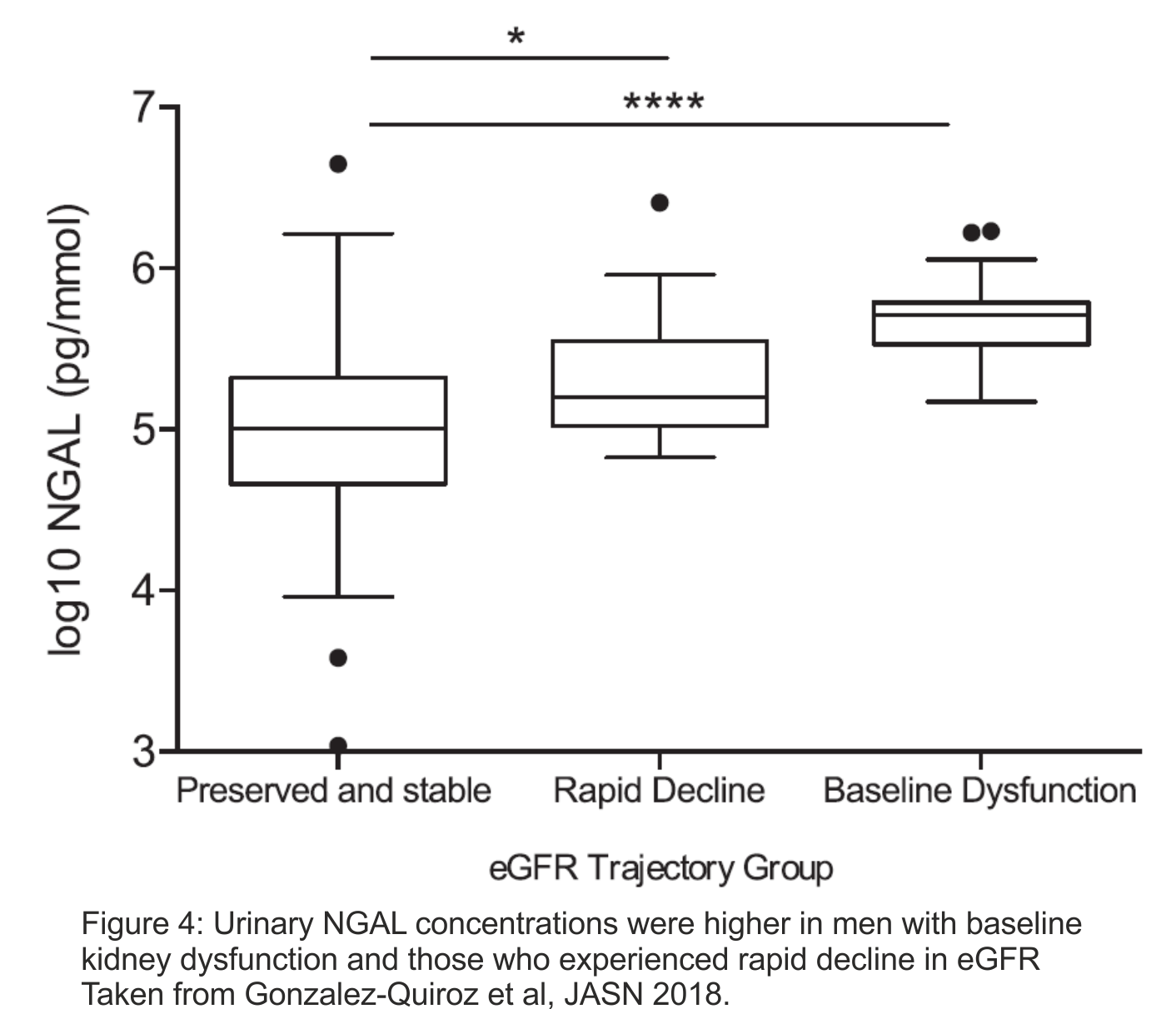
Additionally, 55 samples selected using a nested patient-control approach were analyzed for NGAL.
See here for discussion and explanation of the statistical plan.

Results
520 adults were identified, 4% of the potential participants were excluded because of self-reported CKD, diabetes, or hypertension. 350 participants were included in the study. The study timeline and population participation in depicted in the figure above.
Baseline Renal function in the cohort was as follows.

Baseline demographic data:


eGFR trajectory Groups:
The investigators identified three different subgroups in men and two subgroups in women based on the model intercept (baseline eGFR) and slope (change in eGFR over time).

From the text of the article, "Of the three women who fell into the rapid decline group, one had worked in (nonsugarcane) agriculture, and two worked exclusively at home."
Associations seen with Rapid decline category:
To test whether proposed causal exposures were associated with rapidly declining eGFR trajectory, they conducted age- and educational level–adjusted analyses using probability-weighted logistic regression examining exposures individually using stable with preserved eGFR trajectory as a reference.
Risk factors found to have significant association with rapid declining eGFR
Outdoor work (OR, 10.35; 95% CI, 1.35 to 79.24
(Non-sugarcane) agricultural work OR, 3.57; 95% CI, 1.14 to 11.13
Lack of shade available during work breaks OR, 3.74; 95% CI, 1.59 to 8.76
Risk factors which DID NOT have a statistically significant association with rapid eGFR decline
Years of work in sugarcane
Years of work in agriculture
Self-reported physical effort in the last week at work
Self-reported occupational heat or agrochemical exposure over last 6 months
Alcohol consumption
Self-reported fluid consumption, or water quality or source
Heat/dehydration-related symptoms
Use of nonsteroidal anti-inflammatory drugs
They conducted a sensitivity analysis examining the association with the same rapid decline eGFR trajectory as above and occupational exposures, hydration variables, and heat-related symptoms captured at the second study visit (May 2015; immediately after harvest).
Association was found with –
Working in a sugarcane cutting role OR, 3.84 95% CI, 1.17 to 12.58
Those reporting fever over the last 6 months OR, 5.77; 95% CI, 2.03 to 16.33
No association was found with –
Self-reported measures of heat exposure,
Combined heat-related symptoms,
Fluid intake
Urinary Findings
No associations were found between (baseline) dipstick proteinuria, specific gravity, ACR or eGFR trajectory subgroups. Urinary NGAL levels among men differed between the three outcome startifications.
Discussion
This is the first community-based cohort study from an endemic area of MeN and the first longitudinal study of moderate size with follow-up of at least 6 months from an endemic area. One in ten apparently healthy men (but no women) had evidence of baseline renal dysfunction. One in ten men and and one in thirty-three women had a rapid decline in eGFR.
A recent biopsy study that enrolled patients with established CKDu reported a rate of decline in eGFR of 7.0 ml/min per 1.73 m2 per year among men with a history of sugarcane work.
The only associations with rapid decline in eGFR were the lack of shade and outdoor agricultural work. This emphasizes the importance of working environment as a risk factor in disease progression either by (not reducing) solar exposure or as a surrogate for poor occupational conditions.
None of the other questionnaire responses aimed at capturing heat stress, time-accumulated occupation, or other proposed causes of MeN were associated with the outcome. This raises further questions. Although self-reported measures of thermal sensation and physical exertion have been shown to robustly capture acute physiologic heat stress, these questionnaires may not be valid in capturing heat stress in the rural Nicaraguan population, or they may not reflect time-accumulated heat stress. Or it may be that non-heat-related occupational exposures promote the development of CKDu. An association was found between rapid decline and a cane/seed cutting role (a job role that has been associated with particularly hot working conditions) in a sensitivity analysis examining associations with exposures assessed post-harvest.
Finally, the association between self-reported fever over the previous 6 months at the second study visit and the rapid decline trajectory might support a infectious or inflammatory contributor to CKDu..
Strengths
They avoided probable confounding by associated conditions as they excluded patients with preexisting DM, HTN and CKD.
This enabled them to identify those with aggressive disease and eGFR decline due to CKu.
By excluding patients with preexisting CKD, they eliminated potential issues associated with reverse causation
Limitations
The investigators relied on self-report to quantify most of occupational and environmental exposures. None of questionnaire-based assessments have been validated in the Nicaraguan population.
Resources restricted the study to a moderate sample size; statistical approach was altered. The analytical change lead to a reduction in power.
CKD-EPI formula has not been validated for this population, although this was unlikely to be of major importance as within-person change in eGFR would not be affected by choice of equation.
Those with a rapidly declining renal function did not undergo extensive evaluation. A histopathological correlation would have yielded significant information.
In summary, the study does not provide clear evidence for a cause of the disease. Along with occupation, the importance of non-occupational factors is supported by
The range of jobs undertaken by the men experiencing rapid decline
3.4% of women in our study who also showed a rapid loss of eGFR
The results show striking evolution of disease with a substantial proportion of initially apparently healthy men and a small number of women experiencing rapid loss of kidney function over the 2-year follow-up. Although several occupational risk factors were identified, the range of study participants who sustained loss of eGFR suggests that other factors also play a role. These findings describe a highly prevalent, uniquely aggressive kidney disease with no clear cause
Future and Current Efforts
Balkan nephropathy was the CKDu of the past. It took more than 50 years to ultimately discover the etiological factor (Aristolochia, by the way).
As established, MeN commonly affects poor agricultural communities with the commonest victims being young adults. Thus the social, individual and economic impact is very high. This puts formidable challenges on local health systems. Concerted efforts from clinicians and scientists are needed to identify the etiological factors and subsequently institute corrective and preventive measures.
MeN is the subject of an intensive multidisciplinary effort initiated by several groups including the Pan-American Health Organisation (PAHO), which is the WHO branch for the Americas. In addition, a multi-professional independent consortium denominated CENCAM (Consortium for the Epidemic of Nephropathy in Central America and Mexico), has been established and is now pursuing scientific as well as policy solutions to the Mesoamerican nephropathy epidemic.
Meanwhile, as efforts to understand the disease continue it is important to address potential CKDu risk factors. Examples include water sources that are free of biological and chemical contaminants; work practices that prevent dehydration in workers; and use of accepted safety procedures for agrochemicals.
Summary by Aakash Shingada,
Nephrology Fellow, New Delhi, India
NSMC intern, Class of 2018.